Narrative (P-1)
This patient was visited at my office with a chief complaint of moderate, at times severe pain extending to the right gluteal and posterior thigh and ankle exacerbated by standing or extended periods of walking. The patient reported that the pain was severe enough, that she was unable to continue walking for more than 10 minutes, followed by progressive exacerbation. She has had this complaint for the past 7 months, which was significantly exacerbated during the past 8 weeks.
Previous treatment regiments received included 10 days of complete rest, medications including analgesics, anti-inflammatory including at least two corticosteroid injections, followed by more than 20 sessions of physiotherapy and 20 sessions of hydrotherapy.
However, because of the continuation of her symptoms, particularly the right radicular pain to an extent to prevent her from performing her daily routines, she was consulted by two neurosurgeons. One of whom had recommended surgical intervention.
At the time of her initial examination at my office, the patient presented with a guarded gait. She was able to do heel and toe walk but with difficulty on the right side. SLR was positive on the right at 30 degrees, and the left 55 degrees, causing right-sided pain. Right ankle DTR was reduced with marked hypo-tonicity of right gluteal muscles, and weakness of stabilizers on the right side. Lumbo-sacral range of motion was also significantly reduced in flexion and right lateral flexion.
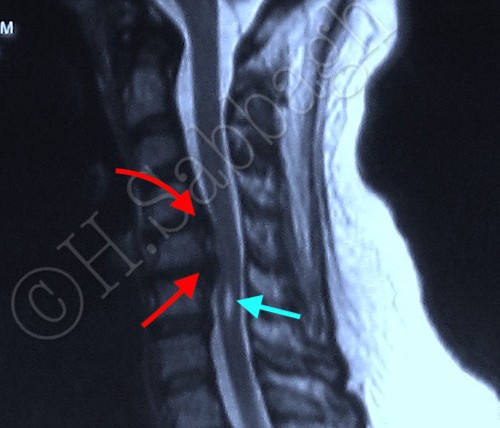
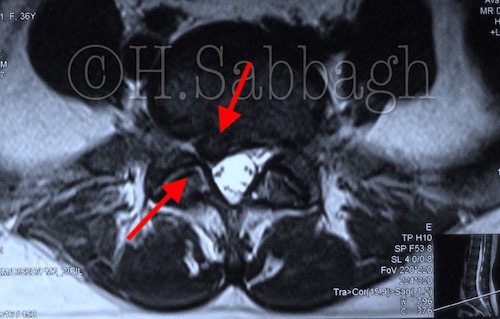
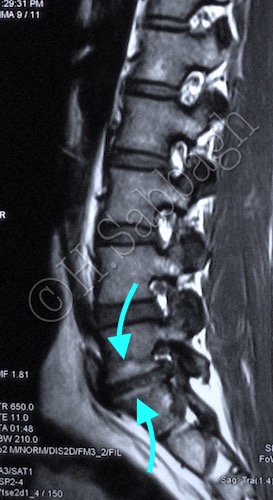
The DPPP-SAA treatment protocol was initiated a few days following the initial examination. The initial (Pre-Treatment) MRI study is available on plates 1-3/10. It confirms L5-S1 lateral right herniation with lateral recess compromise (Red Arrows), corresponding to the patient’s neurological presentation.

Patient response to treatment was slow during the first few sessions. This can be explained by the chronicity of the IVD structural pathology, as well as complications caused by the pre-existing structural retro-listhesis of L5, and Modic type II changes at this level (Cyan Arrows).
It is a clinical fact that the golden period for initiating treatment protocol for IVDs with structural pathology causing neuro-compromise is within the first two weeks of the initial injury. The longer the time passes, the more guarded the prognosis.
Furthermore, degenerative changes affecting the vertebrae end plate seem to directly affect the IVD response to closed reduction protocol.