Narrative
This clinical case review involves a female patient who was referred to a chiropractic office with a chief complaint of insidious neck and upper back pain of a 6 week’s duration. She had denied any radiating pain, with no history of trauma.
Initial examination results are not available.
The patient was referred for plain film radiology study by the attending clinician, which had apparently included two basic views of the cervical spine, APOM, and an AP pelvis plain film study (patient had denied any complaints regarding the lower back or the hip region – Initial plain film study is not available).
Following admission to the Chiropractic treatment program, the patient reported having received three sessions of treatment, which included the use of some modalities followed by Chiropractic cervical rotatory adjustment.
According to the patient, following the initial treatment session she did feel better. However, after the second session, she felt an uncomfortable stiffness in her neck, followed by a gradual onset of left arm pain the next day, both of which were communicated to the treating doctor.
Regardless of the above, the third session of treatment was also performed with further exacerbating results. Apparently, immediately following the last session, she felt a sharp pain in her left arm and shoulder with increasing intensity.
Treatment was discontinued at this stage and the patient consulted an internist who had prescribed analgesics, anti-inflammatory medication, a cervical collar and a referral to my office.
I did visit this patient within twelve days, at which time she reported a significant reduction in her symptoms overall.
At the time of my examination, the cervical spine range of motion was reduced, particularly in left lateral flexion, left shoulder abduction limited and painful, with some spasm and tenderness throughout. DTR was in tact, and muscle testing on the left arm was difficult to evaluate due to resistive pain.
An MRI study of the cervical spine was ordered, the results of which can be seen on plates 1-4.

CR33_PostExac-SagT2 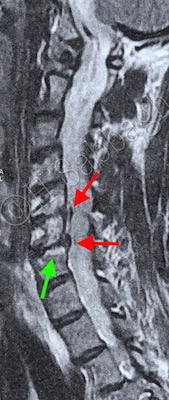
CR33_PostExac-SagT1
Significant degenerative changes include misalignment of C4-5 (Cyan Arrows), bilateral sub-articular disc with osteophytic complex associated with neural foraminal narrowing of C5-6, with extension into the left lateral recess (Red Arrows), modic type II changes to C5-6, and C6-7 segments (Green Arrows).

CR33_PostExac-SagFS 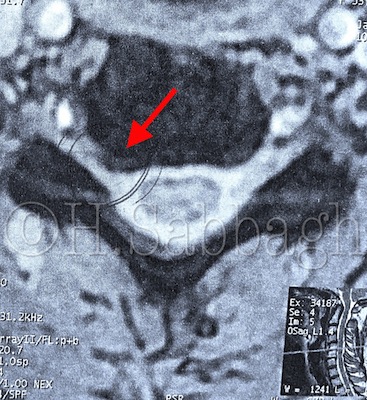
CR33_PostExac-AxT2
The patient was accordingly advised to continue wearing the cervical collar for another 5 days, followed by eventual time reduction.
This patient was re-examined within 2 weeks, at which time her symptoms were reduced significantly, including left arm radicular pain, with a much better range of motion.
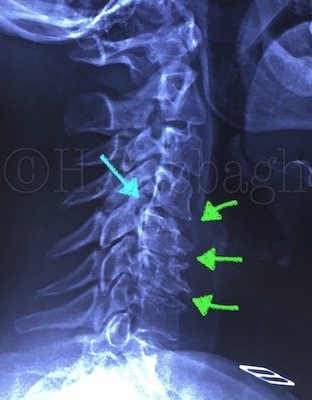
At this stage, a flexion / extension stress study of the cervical spine was also ordered, the result of which can be seen on plate 5-8. Stress study of the cervical spine clearly depicts posterior compartment instability (Cyan Arrows) of the C4-5 segment, in addition to the degenerative changes of the lower segments (Green Arrows).

CR33_PostExac-AP 
CR33_PostExac-Lateral

CR33_PostExac_LatFlex 
Cr33_PostExac-LatExt
Because this patient continued to express some neck and left arm discomfort, she was treated via DPPP-SAA / PDD for four sessions with acceptable results. The patient was also scheduled for a follow up examination within 4 weeks.
Subsequently, the patient was clearly informed regarding the relative instability and degenerative changes to her cervical spine. She was further advised on proper daily ergonomics, and appropriate exercise programs.
