Correlative Neurological Diagnosis
Background
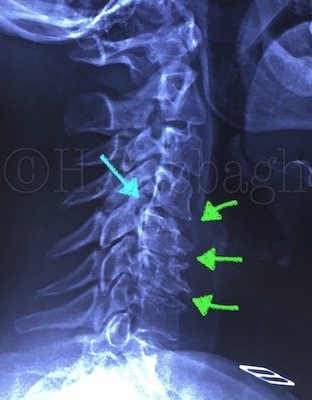
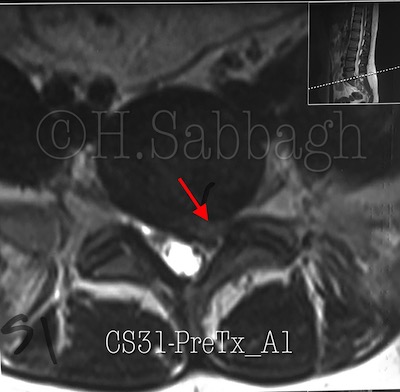
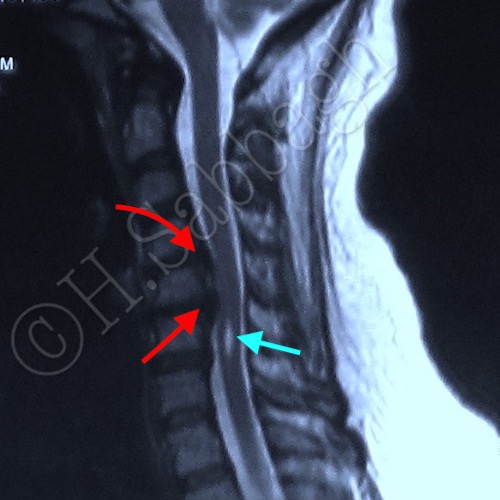
This case represents a 37 years of white female, who presented by bilateral upper extremity pain extending from the cervical spine to C5-6 dermatomal pattern of six months duration. In addition she reported recent episodic tingling and bilateral paresthesia which was exacerbated following receiving more than 20 sessions of physiotherapy treatment including, needling, manual traction, in abscess of a imaging study or even a proper neurological work up by a qualified clinician.
Physical Examination
Vital Sign: P=110 BP=130/85
Neck: Supple – no bruits
Lung: Clear
Heart: Regular no murmur noted
Abdomen: Soft / Non-tender
Extremities: Mild bilateral distal pitting edema right more than left was noted
Neurological Exam: Alert and Orient X 3
Cranial Nerves: Normal / No facial weakness
Cervical ROM: Limited in all ROM, mainly extension exacerbated the numbness and tingling of the upper extremities R > L
Motor Power: Right shoulder abduction 3/5, Left 4/5, Right elbow flexion 4/5/ – Left 5/5, Right Wrist flexion 4/5, Left 5/5, Right hand opposition 4/5/ left 5/5/ Intrinsic Muscles 5/5.
DTR: Right upper extremity, Right BR + Bicep 2+, Left 2/2. Right Tricep 1/2, Left Tricep 2/2.
Coordination and Gait: H/ T walk Ok, Tandem Walk – Ok eyes open/ Romberg Positive.
Sensory: Altered on right upper extremity, pin prick and joint position. Intact light touch.