
Narrative
This clinical case review involved a young patient who was initially admitted to my clinic several yeas ago complaining of low back pain with a history of mild trauma following a fall. At that time, the initial examination found a limited lumbo-sacral ROM, with all other neurological findings within normal limits.
Rest, analgesics, and some restrictions were recommended, and a re-evaluation within one week, in case of inadequate improvement.
Apparently, this patient did not fully recover at that time, but he had referred to another clinician who had recommended an MRI study (Plates 1-2/13). Following the imaging study results which had shown a mild L5-S1 disc bulge, the patient was referred for several sessions of physiotherapy, which had positive results, and he was later released.


Even so, this patient had improved, yet he continued to experience occasional pain, particularly following lifting or demanding exercises such as playing soccer.
He did refer to a third clinician one year later with the same chief complaint. At this stage, a second MRI study was obtained with similar diagnostic results as the previous study (Plates 3-4/13).


Once again, this patient was recommended to undergo a low back injection of corticosteroids, followed by about 20 sessions of physiotherapy.
As a result, and according to the patient, there was significant improvement, and he continued on a more routine exercises program.
Even so, this patient was overall better, he did continue to experience pain during certain activities, with increasing severity. As a result, he referred to a fourth clinician with a similar, but more severe chief complaint three years later.
This patient did undergo a third MRI study (Plates 5-6/13), with similar diagnostic results as the previous two studies. Treatment protocol was also similar to the previous episodes, with temporary relief.


Recently, this patient did return for a second visit to my office (six years from the initial exam) with an exacerbated chief complaint of lower back pain, and in addition to a more recent onset of radiating pain involving the right gluteal region.
Physical examination did confirm significant midline shift during flexion, limited positive SLR, yet intact DTR and muscle strength. The patient did express having experienced limitations and stiffness during bending most of the time during the past several months.
Subsequently, I did order the fourth MRI study which confirmed a pan central L5-S1 protrusion with some compromise of the right lateral recess (Plates 7-8/13). The imaging study findings correlated well with the chief complaint. In addition, there seemed to be a mild anterio-lithesis of L4, instability of which was further confirmed via an S1-Locus Monitoring Instrument (S1LMI).
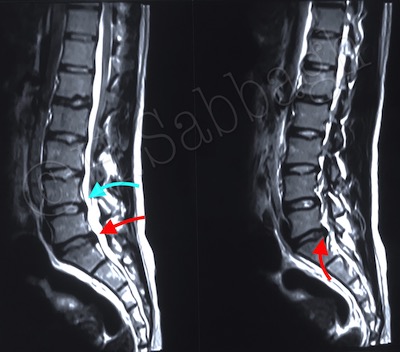

It is important to note that all four MRI studies which were performed several years apart, confirmed the L5-S1 IVD protrusion, and further exacerbation were demonstrated in the most recent study. However, none reported the mild anteriolithesis of L4, or even suggested the possibility of instability in this segment.
During the initial treatment protocol utilizing the S1LMI, further indications of possible instability of L4, consistent with the mild anteriolisthesis noted in the MRI study, were detected.